How is Wilson disease inherited?
Wilson disease is an autosomal recessive disease, which means it occurs equally in men and women. In order to inherit Wilson disease, both parents must carry one genetic mutation (abnormal alteration in the gene) that each parent passes to the affected child. At least one in 30,000 people of all known races and nationalities has the disease.
Of the 23 different human chromosomes, the gene responsible for Wilson disease is located on chromosome 13. The gene is called ATP7B and it contains the genetic information necessary to make a copper transport protein that plays a key role in incorporating copper into ceruloplasmin and moving excess copper out of the liver. Mutations in the gene lead to an abnormal copper transporter that cannot move copper effectively or at all. More than 300 genes of the ATB7B have been identified thus far. This excess copper accumulates in the liver and other organs.
Most patients have no family history of Wilson disease. People with only one abnormal gene are called carriers. Carriers (heterozygotes) may have mild, but medically insignificant, abnormalities of copper metabolism. Carriers do not become ill and should not be treated. Wilson disease patients (homozygotes) do become ill and must receive treatment lifelong or eventually they will develop severe lethal disease.
What is the likelihood of inheriting Wilson disease?
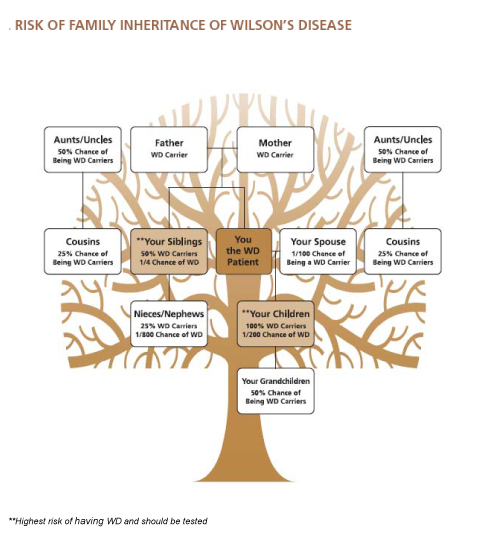
One in 100 individuals in the general population carries one abnormal copy of the Wilson disease gene. Carriers have one normal and one abnormal gene. All (100%) children of those afflicted with Wilson disease receive at least one abnormal copy of the Wilson disease gene. One half (50%) of a carrier's children receive at least one abnormal copy of the Wilson disease gene. This diagram is a basic risk profile for family members. A genetic counselor can provide a more detailed pedigree of specific family relationships.
Family Screening
All siblings and children of Wilson disease patients should be tested for Wilson disease. Other relatives who have had symptoms or laboratory tests that indicate liver or neurological disease also should be tested for Wilson disease.
Biochemical Testing
Children of patient:
· Begin at age 2 if asymptomatic, repeat once in 5 years unless reason to pursue further.
Siblings of patient:
· Physical examination and brief history of any liver or neurological symptoms.
· Liver Function Tests: ALT, AST, Albumin, Bilirubin.
· Ceruloplasmin and Serum Copper.
· 24 hour urine copper
· Slit-lamp exam of the eyes for Kayser-Fleischer rings.
· If no K-F rings, abnormal liver functions tests, and low ceruloplasmin: liver bio
Information about Molecular Genetic Testing
All siblings and children of Wilson disease patients should be tested for Wilson disease. Other relatives who have had symptoms or laboratory tests that indicate liver or neurological disease also should be tested for Wilson disease. More than 300 different mutations of the ATP7B gene have been identified thus far.
Testing Methods Available
Linkage analysis (Haplotype analysis)
Molecular genetic testing to identify a set of closely linked segments of DNA (a marker or set of markers), comparing the markers of family members to those of an affected patient.
Useful for: screening siblings of an identified patient
Gene sequencing (mutation screening of the entire ATP7B gene)
Analysis of the entire ATP7B gene to detect and identify disease causing mutations. An individual with confirmed Wilson disease needs to be tested first. If both mutations are identified, other family members can then be offered testing. Gene sequencing will identify both mutations in most but not all cases of Wilson disease.
Useful for: confirmation of the diagnosis in suspected patients, family members to learn if they could be affected but do not yet have symptoms, to learn they are carriers, or to allow for prenatal testing for confirmed carriers.
Targeted Mutation analysis
Analysis of a specific location in the ATP7B gene for a known particular mutation.
Useful for: specific populations of patients where the common mutations are known; for screening siblings of patients with two identified mutations. Genetic testing is best coordinated through a genetic counselor who can carefully discuss the best method of testing to perform and the benefits, limitations, and implications of each method. Your physician should be able to direct you to a qualified genetic counselor and genetic testing facility.
Genetic testing is best coordinated though a genetic counselor who can carefully discuss the best method of testing to perform and the benefits, limitations, and implications of each method. Your physician should be able to direct you to a qualified genetic counselor and genetic testing facility.

